Introduction
Patient safety is not a theoretical concern—it's a daily life-or-death reality in hospital environments. Between 10% and 12% of hospitalized patients experience adverse events, with roughly half being preventable. These failures carry staggering costs: an estimated $17.1 billion annually in preventable adverse events alone. Beyond the financial toll, hospitals remain among the most hazardous work environments in the United States, with hospital workers experiencing 6.0 nonfatal injuries per 100 full-time employees—double the private industry average.
What drives these outcomes? Leadership behavior is one of the most influential variables in safety outcomes. A 2022 study across 31 hospitals found that a 10-point increase in local leadership scores was associated with:
- 52% lower odds of a concerning safety climate
- 36% lower odds of poor teamwork
- 28% lower odds of staff burnout
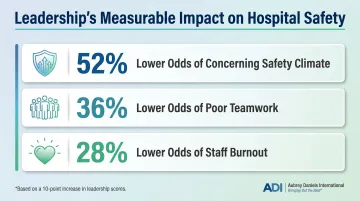
When managers lead safety well, those numbers shift — and patients benefit directly.
Safety leadership team training for hospital managers offers a proven, structured response to this challenge. Unlike individual skill-building programs, team-based training creates a collective, multidisciplinary leadership approach that addresses safety as a systemic responsibility, not a siloed one.
Key Takeaways
- Effective safety leadership training builds multidisciplinary hospital teams that drive systemic improvements together
- Behavior change through practice and reinforcement—not awareness alone—is what separates programs that stick from those that don't
- Fear of error reporting, role ambiguity, and weak institutional support are the most common barriers, and each requires a structural fix
- Training completion rates tell you almost nothing—track behavioral indicators, climate surveys, and patient/staff safety outcomes instead
The Case for Safety Leadership Team Training in Hospitals
Patient safety is inherently systemic. Errors rarely result from a single individual's mistake; instead, they emerge from how teams communicate, prioritize, and respond to risk. This reality makes individual manager training insufficient. Leaders don't operate in isolation—they coordinate across shifts, departments, and disciplines.
Hospital managers occupy a uniquely influential position in shaping safety culture. As first-line safety leaders, they set behavioral norms for their units, model safety values, and determine whether staff feel safe reporting near-misses or errors. Transformational leadership is positively associated with patient safety culture and nursing safety practices, creating environments where safety becomes a shared value rather than a regulatory obligation checked off and forgotten.
What team-based training adds:
Team-based safety leadership training teaches managers from different departments—nursing, operations, pharmacy, facilities, administration—to solve safety problems together. It creates shared accountability and builds the cross-functional relationships necessary for systemic change. A 2011 study published in Health Care Management Review found that learning-oriented, team-based leadership training increased targeted leadership behaviors, promoted a learning orientation, and established new routines among most management groups.
Why hospitals demand this approach:
Hospitals operate under conditions that strain safety culture at every level: high staff turnover, multidisciplinary teams, 24/7 operations, and entrenched hierarchies. Each of these creates friction points where communication breaks down and risk goes unaddressed. One-time workshops cannot produce sustainable change in these settings. Ongoing, structured training builds the behavioral habits that hold up under pressure.
What leadership gaps cost hospitals:
Safety climate deficits directly correlate with increased adverse events, staff injuries, burnout, and regulatory risk. Traditional voluntary reporting missed about 90% of adverse events when compared to active detection methods like the Global Trigger Tool. Leadership failures create silent epidemics of unreported harm, leaving systemic risks undetected until they escalate into serious harm.
Core Components of an Effective Safety Leadership Team Training Program
Learning-Oriented Leadership Behaviors
The most effective programs train managers to model learning behaviors—asking questions, investigating near-misses without blame, and treating failures as improvement data rather than disciplinary triggers. This approach builds psychological safety, a shared belief that the team is safe for interpersonal risk-taking. Evidence shows that psychological safety is associated with lower error rates and improved willingness to speak up about hazards.
How it works in practice:
- Managers learn to respond to near-misses with curiosity, not criticism
- Leaders facilitate root-cause analysis that focuses on systems, not individuals
- Teams conduct non-punitive debriefs after safety events to extract lessons
Behavioral Integrity for Safety
Training must help managers align what they say with what they do. When leaders consistently act in accordance with stated safety values, it builds trust and increases staff willingness to report errors. Research demonstrates strong associations between leadership behaviors and safety climate.
Staff watch what managers prioritize when time is short or resources are limited. Those moments expose where safety actually ranks as a priority — and staff take note.
Signs of behavioral integrity in safety leadership:
- Stopping a task to address a hazard, even under schedule pressure
- Consistently following the same safety protocols expected of frontline staff
- Responding to reported concerns visibly and within a clear timeframe
Communication and Feedback Skills
Communication breakdowns contribute to over 70% of sentinel events reported to the Joint Commission. Training should include practical skill-building in:
- Delivering safety feedback constructively
- Conducting brief safety huddles that engage all team members
- Using structured communication tools like SBAR/ISBAR
Implementing SBAR-based communication toolkits reduced mean time to treatment in one medical ICU from 7.19 to 3.69 minutes and improved nurse satisfaction.
Behavior-Based Reinforcement Strategies
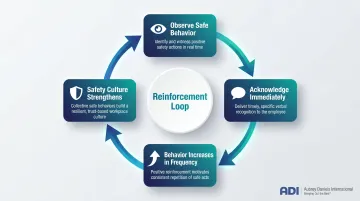
Communication tools improve information flow — but sustaining safe behavior requires a different mechanism: reinforcement. Programs grounded in behavioral science teach managers to use positive reinforcement, recognizing and rewarding safe behaviors in real time, rather than relying solely on rule enforcement. This approach shifts safety from a compliance activity to a reinforced organizational habit.
ADI's Judy Agnew, co-author of Safe by Accident, points out that sustainable safety culture depends on leadership practices that systematically reinforce desired behaviors. When managers catch staff doing safety-conscious work and acknowledge it immediately, those behaviors increase in frequency. When safety only surfaces during audits or after incidents, the reinforcement signal is absent — and behavior drifts accordingly.
Multidisciplinary Team Exercises and Role Clarity
Effective training brings together managers from nursing, operations, pharmacy, facilities, and administration to work through real safety scenarios. This approach:
- Clarifies role boundaries and reduces ambiguity
- Builds cross-functional relationships needed for systemic problem-solving
- Ensures safety decisions aren't made in departmental silos
When every role has a defined safety responsibility — and those definitions are tested under realistic scenario conditions — coverage gaps surface before they become incidents.
Best Practices for Implementing Team-Based Safety Leadership Training
Conduct a Gap Analysis Before Designing Training
Successful programs start with a structured gap analysis to identify where leadership behaviors are weakest, what safety reporting data reveals, and how current training stacks up against recognized benchmarks like OSHA or Joint Commission standards.
Why off-the-shelf programs fail:
Generic training ignores the specific challenges your organization faces. A gap analysis uncovers local barriers—whether it's poor handoff communication between shifts, fear of reporting in certain units, or unclear escalation protocols for rapid response. Programs tailored to these realities produce measurable behavior change. Generic programs don't.
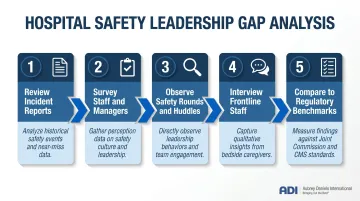
How to conduct a gap analysis:
- Review safety incident reports and near-miss data for patterns
- Survey staff and managers using validated tools (AHRQ Hospital Survey on Patient Safety Culture)
- Observe safety rounds, huddles, and handoffs to identify communication breakdowns
- Interview frontline staff about perceived leadership support for safety
- Compare current practices to regulatory standards and industry benchmarks
Building a Multidisciplinary Leadership Team
Once you know where the gaps are, structure the training cohort to address them cross-functionally. Include department heads, charge nurses, clinical leads, and administrative managers together — siloed training reinforces siloed thinking. Representation should include:
- Nursing leadership (charge nurses, nurse managers, CNOs)
- Clinical department heads (pharmacy, laboratory, imaging)
- Operations and facilities managers
- Quality and risk management leaders
- Frontline supervisors with direct staff oversight
Why senior leadership sponsorship matters:
Training succeeds when hospital executives visibly participate, set clear expectations, and allocate dedicated time and resources. Joint Commission standards require leaders to create and maintain a culture of safety, regularly measure it, and align organizational priorities accordingly. Without executive sponsorship, middle managers deprioritize training when operational pressures spike.
Designing Training That Changes Behavior
Distinguish awareness from behavior change:
Many safety training programs fail to produce lasting change because they stop at awareness. Participants learn what they should do — not how to do it consistently under real-world pressure. Effective programs use:
- Repeated practice of specific skills (giving safety feedback, conducting huddles)
- Scenario-based exercises that simulate actual unit conditions
- Structured follow-through with clear behavioral expectations
- Observation and feedback on real leadership behaviors post-training
Sustaining behavior change after training:
The most effective programs include follow-up coaching, team debriefs after safety events, and regular review of behavioral metrics. What managers practice in the classroom erodes quickly without reinforcement on the floor — consistent feedback loops are what convert training into habits that hold under pressure.
Overcoming Common Barriers to Safety Leadership Training in Hospitals
Fear of Error Reporting
Many managers and staff underreport near-misses because of fear of blame or professional consequences. Systematic reviews identify fear of punishment as a dominant barrier to reporting. Training must explicitly build psychological safety by:
- Establishing non-punitive reporting norms in policy and practice
- Modeling non-blame communication at the leadership level
- Separating system improvement from individual discipline
- Celebrating reporting as a sign of vigilance, not failure
Implementing Just Culture principles in one hospital increased patient safety event reporting by 37.31% and improved perceptions of leadership response from 30% to over 60%.
Role Ambiguity and Unclear Responsibilities
When clinical leads, charge nurses, and department managers share overlapping responsibilities, safety actions fall through the gaps. A role clarification component in training directly addresses this by:
- Define specific safety behaviors expected of each leadership position
- Map accountability for safety activities (huddles, rounds, incident follow-up)
- Clarify escalation pathways and decision authority
- Document agreements in writing and review regularly
Institutional Barriers
Beyond individual and team-level barriers, hospital managers frequently cite limited time, resource constraints, and lack of executive endorsement as structural roadblocks. Building a business case for training investment means framing safety in terms executives already prioritize:
- Frame safety training as risk reduction—preventing one never event saves far more than training costs
- Link training to accreditation readiness (Joint Commission leadership standards require safety culture measurement)
- Present safety culture improvement as a staff retention strategy (burnout correlates with poor safety climate)
- Use benchmarking data to show gaps between your organization and high-reliability peers

Measuring Success and Sustaining a Safety Leadership Culture
Multi-Level Measurement Approach
Program effectiveness should be measured at three levels:
1. Behavioral indicators:
- Did managers change how they conduct safety rounds?
- Are managers delivering constructive safety feedback weekly?
- Have safety huddles become routine on all units?
2. Climate indicators:
- Did staff perceptions of safety culture improve on validated surveys?
- Tools include AHRQ Hospital Survey on Patient Safety Culture (HSOPS) and Safety Attitudes Questionnaire (SAQ)
- Track composites like supervisor support for safety, communication openness, and reporting culture
3. Outcome indicators:
- Did adverse event rates decline?
- Did near-miss reporting frequency increase (a positive sign of improved reporting culture)?
- Did staff injury rates or patient harm indicators improve?
Sustainability Requirements
Safety leadership culture erodes without ongoing reinforcement. Sustainability requires:
- Coaching structures: Assign executive coaches or peer mentors to support managers post-training
- Peer accountability: Create multidisciplinary safety leadership councils that meet regularly
- Regular leadership safety walk-rounds: Schedule weekly or biweekly unit visits focused on listening and learning
- Certification renewal: Require periodic recertification to refresh skills and update practices
- Integration into performance evaluation: Include specific safety leadership behaviors in manager reviews
One-time training events create temporary awareness; sustained programs build consistent habits. TeamSTEPPS implementation reduced perioperative deaths from 0.069% to 0.019% and unscheduled reoperations from 0.24% to 0.11% — concrete evidence that structured, team-based training produces measurable clinical outcomes when applied with fidelity.
For hospital managers building a behavior-based safety leadership program, ADI's consulting services, certification programs, and resources — including Judy Agnew's Safe by Accident — apply over 45 years of behavioral science to help healthcare organizations move beyond compliance training toward durable culture change.
Frequently Asked Questions
What is safety leadership training?
Safety leadership training is a structured development program that teaches managers and team leaders the specific behaviors, communication practices, and decision-making skills needed to build and sustain a safe work environment. In hospitals, it extends beyond compliance to actively shaping safety culture through leadership actions.
What is the role of safety leadership and team?
Safety leadership involves modeling safe behaviors, enabling open error reporting, and driving systemic improvement. The team's role is to carry out safe practices, communicate hazards proactively, and participate in the feedback loop that makes safety a genuine shared value, not just a compliance requirement.
What are the 7 pillars of patient safety?
The Seven Pillars framework developed at the University of Illinois includes: event reporting, investigation, communication and disclosure, rapid resolution/remediation, system improvement, data tracking/analysis, and education/training. Strong safety leadership supports each pillar by establishing the behavioral norms and accountability structures that make these processes work at the unit level.
What are the 7 basics of team leadership?
Foundational team leadership principles relevant to hospital managers include clear communication, role clarity, psychological safety, accountability, shared goals, continuous feedback, and recognition. Each maps directly to safety leadership: clarifying roles reduces errors, building psychological safety increases reporting, and consistent feedback reinforces safe practices in real time.