Introduction
According to the MedPAC March 2026 Report, approximately 6,436 Medicare-certified ASCs operated in the United States in 2024 — performing 6.4 million fee-for-service Medicare procedures annually, with volume growing over 2% per year between 2019 and 2024.
More procedures, more complex cases, and leaner staffing models mean that the margin for safety failures has shrunk — not grown.
Yet most ASC safety efforts focus on policies, checklists, and accreditation compliance — and adverse events persist. The gap is not in documentation; it's in the daily safety behaviors of staff and leaders that policies alone cannot change. Surgical checklists exist, but staff skip steps under time pressure. Reporting systems are in place, but only 2.5% of patient safety events in the national database come from outpatient settings, suggesting systematic underreporting.
The missing piece isn't more policy — it's changing the daily behaviors that policies were meant to produce in the first place.
TLDR
- Safety culture rests on three pillars — environmental structures, staff attitudes, and individual behaviors — and all three must align
- Compliance tools set a baseline but don't change behavior on their own — reinforcing the right actions does
- Leadership must visibly model safe behaviors daily through observation rounds, immediate feedback, and constructive incident response
- The AHRQ ASC Survey on Patient Safety Culture is the validated tool for assessing culture and tracking progress over time
- High near-miss reporting rates signal a healthy culture — shift from punishing errors to reinforcing safe behavior
What Is Safety Culture in an ASC?
Defining Safety Culture vs. Safety Climate
AHRQ's Patient Safety Network defines patient safety culture as "the values, beliefs, and norms that are shared by healthcare practitioners and other staff throughout the organization that influence their actions and behaviors." Safety culture represents the underlying organizational values; safety climate is how those values are perceived by teams at a specific moment in time.
The distinction matters for leaders. Climate can fluctuate week-to-week based on workload or staffing, while culture represents the deeper behavioral patterns that require years to shift.
The Three-Part Model
The Institute of Medicine framework identifies three organizational elements that create safety culture:
- Environmental structures and processes — physical design, staffing models, technology, protocols
- Staff attitudes and perceptions — beliefs about safety priority, trust in reporting systems, psychological safety
- Individual safety behaviors — how staff actually perform procedures, communicate risks, and respond to errors

Excellent policies (structure) mean nothing if staff don't believe reporting is safe (attitude) or continue cutting corners under pressure (behavior). All three elements must reinforce each other.
What Makes ASCs Structurally Distinct
ASCs differ from hospitals in ways that amplify safety culture challenges:
- Same-day care model — patients arrive, undergo procedures, and discharge within hours, compressing decision windows
- Lean staffing — fewer personnel per procedure creates workload pressure
- Rotating providers — surgeons and anesthesia teams vary daily, disrupting communication norms
- High procedure volume — throughput pressure can normalize shortcuts
These structural realities mean that tools designed for hospital settings rarely translate well. The AHRQ ASC SOPS survey was developed specifically because hospital safety tools didn't adequately address the ASC environment — standard frameworks assume stable teams, extended patient stays, and buffer capacity, none of which apply in most ASCs.
Key Elements of a Strong Safety Culture in an ASC
Psychological Safety and Error Reporting
A functioning safety culture depends on staff willingness to report errors and near-misses without fear of punishment. The 2021 AHRQ ASC SOPS Database Report found that while 85-91% of staff rated their facility "Excellent" or "Very Good" overall, this perception masked a critical gap: doctors/surgeons reported 98% positive communication openness, while support staff reported only 83%. This hierarchy-driven disparity is dangerous — it means frontline staff who witness risks may not feel safe speaking up to physicians.
Psychological safety looks like this behaviorally:
- Staff interrupt procedures when they notice a safety concern
- Mistakes are disclosed immediately, not concealed
- Near-misses are treated as learning opportunities, not disciplinary triggers
- All team members — regardless of role — feel equally empowered to raise issues
When this element is missing, ASCs operate in a state of invisible risk: problems exist but remain unreported until they cause patient harm.
Teamwork, Communication, and Structured Protocols
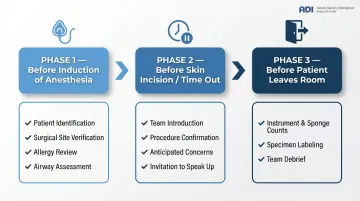
Closing that reporting gap requires more than culture — it requires structure. Structured communication tools reduce reliance on informal norms and prevent errors. The Ariadne Labs Ambulatory Safe Surgery Checklist covers three surgical phases:
- Before Induction of Anesthesia — patient ID, site verification, allergy review, airway assessment
- Before Skin Incision (Time Out) — team introduction, procedure confirmation, anticipated concerns, invitation to speak up
- Before Patient Leaves Room — instrument/sponge counts, specimen labeling, team debrief on recovery concerns and improvement opportunities
Systematic reviews associate surgical checklists with increased hazard detection, decreased complications, and improved team communication. Checklists only work when leadership enforces them consistently — not selectively under time pressure.
Leadership Commitment and Staff Competency
Leadership commitment must be demonstrated daily, not just through policy endorsements. When a charge nurse skips a safety step to save time, every staff member watching learns that efficiency outranks safety.
Staff competency requires:
- Ongoing training beyond annual compliance modules
- Simulation drills for critical events (malignant hyperthermia, cardiac arrest, airway emergency)
- Annual competency assessments as required by accreditation standards
Regulatory requirements set the baseline. CMS regulation 42 CFR 416.43 requires ASCs to maintain QAPI programs covering adverse event tracking, root cause analysis, and a governing body mandate to "clearly establish expectations for safety."
The Joint Commission's 2026 National Patient Safety Goals add further requirements:
- Two-patient identifiers before every procedure
- Medication labeling on sterile fields
- Medication reconciliation
- Hand hygiene compliance
- Universal Protocol (preprocedure verification, site marking, time-out)
Meeting these standards is necessary — but ASCs that treat compliance as the finish line miss the deeper work of behavior change that makes safety stick between audits.
Why Rules and Checklists Alone Don't Build Safety Culture
The Behavioral Science Gap: Antecedents vs. Consequences
Policies, training, and checklists are antecedents — they prompt behavior but cannot sustain it. Behavioral science research demonstrates that consequences determine whether behavior persists. When unsafe behavior produces immediate positive consequences (saved time, convenience) while safe behavior produces delayed or uncertain consequences (avoiding a rare adverse event), antecedents alone will fail.
The more immediate and certain a consequence, the more powerful its effect on behavior.
The Compliance Trap
ASCs often fall into the "compliance trap": staff follow procedures when observed or under heightened scrutiny (accreditation surveys, incident investigations), but revert to shortcuts when consistent reinforcement is absent. Behavioral science predicts exactly this pattern.
As Judy Agnew and Aubrey Daniels document in Safe by Accident, a low injury rate can be misleading — organizations may appear safe while risky behavioral patterns accumulate undetected. They advocate shifting from lagging indicators (incident rates) to leading indicators (behavioral observations), and from negative reinforcement to positive reinforcement of safe behaviors.
Normalization of Deviance
Published research documents how healthcare workers rationalize protocol deviations until unsafe practices become routine. Examples include:
- Surgeons continuing with contaminated instruments
- Anesthesiologists disabling safety alarms
- Nurses sharing medication dispensing passwords to bypass witness requirements
Staff justify rule-breaking as being "for the good of the patient" or because rules are perceived as "stupid and inefficient." A VitalSmarts/AACN study of over 1,700 healthcare professionals found it was "between difficult and impossible" to confront colleagues about rule-breaking.
This phenomenon is amplified in high-volume, lean-staffed ASC environments where production pressure is constant.
The Missing Ingredient: Positive Reinforcement
Normalization of deviance thrives where safe behavior goes unnoticed. When leaders specifically acknowledge safe behaviors in the moment — not just track lagging indicators like incident counts — those behaviors become reliable habits. A surgeon who gets verbal recognition for pausing to verify a timeout is more likely to pause again tomorrow than one whose compliance is recorded only in an audit spreadsheet.
The Just Culture Model
The Just Culture framework gives ASC leaders a principled basis for responding to safety events — one that builds rather than erodes reporting culture. It distinguishes three categories:
| Category | Definition | Leadership Response |
|---|---|---|
| Human error | Unintentional mistake | Redesign the process or system |
| At-risk behavior | Shortcut with perceived benefit | Coach and reinforce correct behavior |
| Reckless behavior | Conscious disregard for safety | Apply accountability measures |

The Role of Leadership in Building ASC Safety Culture
The Role of Leadership in Building ASC Safety Culture
Walk-the-Talk Leadership
Culture is set at the top but maintained by the daily behavior of charge nurses, lead surgeons, and managers who either reinforce or unknowingly undermine safe practices. When a leader skips a safety step to save time, they communicate to every staff member watching that efficiency outranks safety.
A 2023 systematic review found leadership walkarounds positively associated with:
- Improved safety climate scores
- Increased near-miss reporting frequency
- Increased understanding of safety initiatives
- Reduced provider burnout
Direct leader presence on the clinical floor is among the most evidence-supported interventions.
The Principle of Immediacy
Leaders who provide specific, positive feedback immediately when they observe safe behavior create far stronger and more durable behavioral change than those who wait for annual reviews. Behavioral science establishes that consequences that are soon, certain, and positive have the strongest effect on behavior.
Example: A manager who verbally recognizes a nurse for completing a pre-procedure checklist correctly creates a more powerful consequence than a quarterly safety award.
Reinforcing safe behavior is only half the equation. How leaders respond when things go wrong matters just as much.
The First Error Sets the Template
A leader's response to the first reported error or near-miss sets the template for all future reporting in the facility. A punitive or dismissive reaction can shut down an ASC's reporting culture for years; a constructive, visible response signals that it is safe — and valuable — to come forward.
Embed Safety into Daily Routines
Leaders should normalize safety conversations by integrating them into:
- Pre-procedure huddles
- Structured post-case debriefs
- Regular safety metric reviews at team meetings
When safety is woven into existing workflows rather than added on top of them, staff begin to treat it as part of how clinical work gets done — not an interruption to it.
Practical Strategies to Improve Safety Culture in Your ASC
Start with a Validated Safety Culture Assessment
Administer the AHRQ ASC Survey on Patient Safety Culture as the starting point. It is validated, free, and provides benchmarking data against national ASC averages across dimensions including teamwork, communication, error reporting, leadership, and staffing.
To get accurate baseline data:
- Ensure high participation rates through protected time and leadership endorsement
- Guarantee anonymity through third-party administration or secure online platforms
- Communicate clearly that the survey is for improvement, not punishment
The 2025 database includes data from 292 ASCs, enabling comparative analysis.
Implement Structured Communication and Checklist Protocols
Adopt surgical safety checklists adapted for ASC workflows, standardized SBAR handoff protocols, and non-negotiable pre-procedure timeouts. These tools only work when leadership enforces them consistently — not selectively under time pressure.
Key protocols:
- Pre-induction checklist (patient ID, allergies, site marking)
- Pre-incision timeout (entire team confirms procedure, site, patient)
- Pre-discharge checklist (counts, specimens, recovery handoff)
- Standardized handoff communication using SBAR format

Build a Behavior-Based Reinforcement System for Safety
Checklists enforce compliance — but building a lasting safety culture requires moving from reactive safety management to proactive safety leadership that actively reinforces safe behaviors.
Leaders should:
- Regularly conduct brief safety observation rounds
- Provide specific positive feedback when they see safe practices performed
- Track leading indicators (near-miss reports submitted, checklist completion rates) not just lagging ones
ADI applies this reinforcement-driven approach with healthcare clients, helping leaders build the observation and feedback habits that sustain culture change over time.
Establish Non-Punitive Incident and Near-Miss Reporting
Components of an effective reporting system:
- Anonymous reporting options (phone hotline, online form, drop box)
- Rapid acknowledgment of every report
- Visible follow-through on concerns raised
- Regular feedback to staff on what changed as a result of their reports
More near-miss reports signal a healthier culture — not more problems. When staff feel safe reporting, you gain visibility into risk before it reaches patients.
Commit to Regular Simulation and Competency Reinforcement
Annual competency assessments should be supplemented with scenario-based simulation drills for high-stakes, low-frequency events:
- Malignant hyperthermia
- Cardiac arrest
- Difficult airway
- Anaphylaxis
- Fire in the OR
Simulation builds behavioral fluency: the ability to respond automatically and correctly under pressure, not just recall what a written procedure says.
How to Measure and Sustain Safety Culture Improvements
Leading vs. Lagging Indicators
A complete measurement system requires both:
| Indicator Type | Examples | Strength | Limitation |
|---|---|---|---|
| Leading (Proactive) | Near-miss reporting rate, checklist compliance %, SOPS composite scores, behavioral observation rates | Predicts future risk; actionable before harm occurs | Requires consistent measurement infrastructure |
| Lagging (Reactive) | Wrong-site surgery rate (ASC-3), sentinel events, adverse event counts, SSI rates | Easy to track; regulatory requirement | Rare events provide false reassurance; too late for prevention |
For ASC leaders, the practical implication is this: a clean lagging record doesn't mean safe conditions exist. The national wrong-site surgery rate of 0.036 per 1,000 procedures looks reassuringly low on paper — but that number can coexist with staff routinely skipping timeout steps, checklist compliance eroding, and near-misses going unreported. Leading indicators surface those gaps before a sentinel event forces attention.
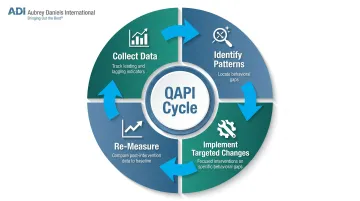
The QAPI Cycle as the Sustainability Engine
The QAPI cycle creates ongoing improvement:
- Collect data — track both leading indicators (near-miss rates, checklist compliance) and lagging indicators (adverse events, ASC-3 metrics)
- Identify patterns — where are behavioral gaps?
- Implement targeted changes — address specific behavioral gaps with focused interventions (e.g., observed timeout compliance in one OR suite) rather than facility-wide mandates
- Re-measure — compare post-intervention data against baseline to confirm whether the behavioral change held
Re-administering the AHRQ ASC SOPS survey annually or biannually allows leaders to track cultural shifts and benchmark against national peers.
Realistic Expectations
The QAPI cycle is designed to run continuously — which is why the timeline for meaningful cultural change is longer than most leaders expect. The IOM estimates approximately 5 years to develop a genuine culture of safety in a healthcare organization. AHRQ recommends measuring safety culture on a yearly basis to track incremental progress against that horizon.
ASC leaders should plan multi-year improvement trajectories with annual benchmarking. Sustainability requires embedding reinforcement into daily operations — not treating safety as a time-boxed project.
Frequently Asked Questions
What are the key elements of safety culture in an ambulatory surgery center?
Safety culture has three core pillars: environmental structures and processes (staffing, protocols, technology), staff attitudes and perceptions (psychological safety, trust), and individual safety behaviors (actual performance under pressure). All three must work in alignment to produce genuine safety culture rather than surface-level compliance.
How can safety culture be improved in an ambulatory surgery center?
Start with the AHRQ ASC SOPS survey to establish a cultural baseline, then reinforce safe behaviors through immediate positive feedback rather than rules alone. Pair that with non-punitive error reporting and leadership that visibly models safe practices through daily walkarounds and structured observation.
What is a Just Culture framework and why does it matter for ASCs?
Just Culture distinguishes between human error (requiring system-level response), at-risk behavior (requiring coaching and reinforcement), and reckless behavior (requiring accountability). This enables fair, consistent responses that protect the reporting culture rather than suppressing it.
How do you measure safety culture in an ambulatory surgery center?
Use the AHRQ ASC Survey on Patient Safety Culture (ASC SOPS) as your primary validated tool, supplemented by leading indicators like near-miss reporting rates and protocol compliance. Re-administer SOPS annually to track cultural shifts and benchmark against national ASC averages — not just at accreditation intervals.
Why do safety culture improvement efforts often fail in ASCs?
Most efforts invest heavily in antecedents — training, checklists, policies — while neglecting consistent reinforcement of safe behaviors. Without reinforcement, compliance is contingent on oversight and fades when pressure lifts. Behavioral science shows that immediate, positive consequences sustain behavior far more effectively than delayed, uncertain consequences like avoiding rare adverse events.
What role does staff error reporting play in ASC safety culture?
Near-miss and error reporting is both a leading indicator of a healthy culture and a primary driver of improvement. ASCs with high voluntary reporting rates, supported by non-punitive systems, have more opportunities to identify and fix systemic vulnerabilities before they cause patient harm. A high reporting volume means staff trust the system enough to speak up — that trust is what makes improvement possible.