Introduction
Many organizations face the same frustrating reality after completing a safety culture survey: they have valuable data about employee perceptions, incident reporting patterns, and leadership support—but no clear roadmap for turning those insights into meaningful change. Surveys collect insights, but action plans are what actually transform culture.
Without a structured response, what was intended as a diagnostic tool becomes a missed opportunity. Employee trust erodes when staff invest time in honest feedback but see nothing change. Participation rates decline in future surveys, and one systematic review identified survey fatigue and lack of visible follow-through as primary barriers to response rates.
Meanwhile, the safety gaps the survey identified keep compounding, creating both operational risk and regulatory exposure.
Turning survey results into a working action plan requires more than a to-do list. It demands leadership alignment, an understanding of what actually drives safe behavior, and the cross-functional coordination to address root causes rather than surface symptoms. This guide covers each step of that process — from interpreting your survey data to building accountability structures that sustain change over time.
Key Takeaways
- A safety culture survey action plan turns survey data into prioritized, behavior-focused initiatives with clear owners and deadlines
- Start with root cause analysis of low-scoring dimensions, not symptom-level fixes
- Leadership visibility and transparent communication of results maintain employee trust and participation
- Assign specific owners, set measurable goals, and schedule re-measurement — without these, nothing changes
- Sustained improvement comes from consistent reinforcement of safe behaviors, not one-time training
What Is a Safety Culture Survey Action Plan (and Why Most Fail)
A safety culture survey action plan is a structured, documented response to survey findings that identifies priority areas, sets improvement goals, assigns ownership, and schedules reassessment. Unlike a generic corrective action plan—which typically addresses isolated process failures—a safety culture action plan targets the shared beliefs and behaviors that shape how an entire organization approaches risk, reporting, and accountability.
Understanding which beliefs and behaviors to target requires a framework. James Reason's 1997 framework identified four interdependent subcultures that together constitute an "informed culture":
The Four Pillars of an Informed Safety Culture
- Reporting culture — Do employees feel psychologically safe reporting errors, near-misses, and unsafe conditions?
- Just culture — Are accountability practices fair, distinguishing between human error, at-risk behavior, and reckless conduct?
- Flexible culture — Can authority patterns and decision-making adapt during safety-critical moments?
- Learning culture — Does the organization systematically act on the safety information it collects?

These dimensions commonly appear in validated tools like AHRQ's Hospital Survey on Patient Safety Culture (HSOPSC), which has been used by thousands of hospitals globally since its release in 2004. A good action plan must address deficits in these specific subcultures rather than treating safety culture as a monolithic entity.
Why Most Action Plans Fail
Most action plans list activities—"conduct training," "update policies," "hold safety meetings"—without changing the behavioral conditions that produced the problem in the first place. AHRQ's Action Planning Tool identifies three primary failure modes:
- Trying to address too many areas simultaneously rather than focusing resources on one or two high-impact priorities
- Assigning no individual accountability—the plan lists initiatives but no named owner drives execution
- Never re-measuring outcomes—staff perceive that survey results were collected but ignored
Avoiding these failure modes means shifting focus from activities to outcomes—specifically, the reinforcement patterns and behavioral conditions that determine whether any initiative actually sticks.
Before You Build: Prerequisites and Key Considerations
Before building your action plan, verify that three foundational elements are in place:
- Valid, department-level data with adequate response rates. AHRQ recommends a minimum 50% response rate; a 2022 systematic review found the actual average was 66.5%. Electronic-only surveys average 54.8%, compared to face-to-face (71.7%) or paper (68.3%).
- Visible leadership commitment. Senior leaders need to understand what's at stake — business risk, operational impact, regulatory exposure — before committing resources. Without executive sponsorship, action plans stall regardless of how well they're designed.
- A cross-functional improvement team with frontline staff, supervisors, and safety/HR leads. Management consistently reports more positive safety perceptions than frontline workers, so planning without frontline representation will miss critical vulnerabilities.
Psychological Safety and Confidentiality
If staff believe survey results can be traced back to individuals, data may be skewed and future participation will decline. Fear of punitive consequences blocks honest reporting. Organizations should verify their survey methodology produced reliable, unbiased results—through confidential administration, third-party data handling, and clear communication about anonymity—before treating scores as actionable.
Benchmark Your Results
Compare your scores against:
- Internal departments/units to identify where gaps are most significant
- External industry baselines using AHRQ's five national comparative databases (Hospital, Medical Office, Nursing Home, Community Pharmacy, Ambulatory Surgery Center)
Benchmarking reveals which dimensions represent the greatest risk and where improvement will have the highest impact. A behavior-based safety assessment, like those ADI delivers, can establish a measurement baseline and provide a behavioral science lens for interpreting what scores actually mean for day-to-day performance.
How to Build a Safety Culture Survey Action Plan: Step-by-Step
The process follows a clear sequence: analysis → prioritization → goal-setting → intervention design → ownership assignment → documentation. Shortcuts in early stages—especially skipping root cause analysis—lead to surface-level fixes that do not change culture.

Step 1: Analyze and Prioritize Survey Findings
Go beyond top-line composite scores. Break results down by:
- Department and work area
- Role (management vs. frontline)
- Shift or team
Safety culture perceptions consistently vary by position and work area. Management typically reports more positive perceptions than frontline workers, so aggregate scores can mask vulnerabilities.
Apply a prioritization lens. Not every low score requires equal urgency. Focus first on dimensions where:
- Low scores intersect with high safety risk (e.g., nonpunitive response to error in high-hazard areas)
- The gap between management and frontline perceptions is widest
- The dimension is a strong predictor of key outcomes
AHRQ's pilot study found that Hospital Management Support for Patient Safety was the strongest predictor of Overall Perceptions of Safety, while Feedback and Communication About Error was the strongest predictor of Frequency of Event Reporting. Prioritize dimensions with demonstrated predictive power for outcomes you care about.
Step 2: Conduct Root Cause Analysis Before Selecting Interventions
Low scores are symptoms. Your action plan must address underlying behavioral causes.
For example, low scores on "communication openness" may not stem from a lack of communication skills training. The root cause might be punitive leadership responses to error—employees have learned that speaking up leads to negative consequences, so they stay silent.
Use team-based root cause discussions:
- Apply the 5 Whys methodology to drill down from symptoms to root causes
- Identify what antecedents (conditions before behavior) and consequences (outcomes following behavior) are driving unsafe behaviors or silence
- Avoid the trap of assuming training is always the answer
- Involve frontline workers directly — they know what's actually happening on the floor
A study in Safety and Health at Work documented a cement manufacturing company where training, audits, and awareness campaigns were "inadequate in reaching their safety target." Only after implementing behavior-based interventions did total accidents drop from 845 to 396 and injuries from 146 to 54.
Step 3: Set SMART Improvement Goals Tied to Specific Dimensions
Each priority dimension needs a specific, measurable goal. AHRQ's Action Planning Tool explicitly recommends SMART goals: Specific, Measurable, Achievable, Relevant, and Time-bound.
Good goal:
"Increase the percent-positive score on Communication Openness in Unit X from 42% to 65% by December 2026."
Bad goal:
"Improve safety communication."
Ground each goal in your current baseline score and a benchmarked target. If the industry average for Communication Openness is 68% and your unit scored 42%, a target of 65% within 12-18 months is ambitious but achievable.
Step 4: Design Behavior-Focused Interventions
Interventions must target behavior change, not just awareness. The most effective interventions combine:
Changes to antecedents (conditions that precede behavior):
- Structured safety briefings at shift start
- Visual cues and checklists at high-risk task points
- Clear role definitions for reporting near-misses
Changes to consequences (outcomes following behavior):
- Leadership visibly acknowledging near-miss reports
- Positive reinforcement when employees speak up about safety concerns
- Responding to error reports constructively, without blame or punishment
One-time training programs rarely sustain culture change. What sustains it is consistent reinforcement of new safe behaviors. Research across 88 international sites found that behavior-based safety implementation produced average injury reductions of 25% in Year 1, 34% in Year 2, and 42% in Year 3—sustained improvement came from continuous behavioral observation, feedback, and positive reinforcement, not from initial training alone.

ADI's work in this area—spanning over 45 years of applied behavior analysis across manufacturing, energy, mining, and other high-hazard industries—focuses specifically on identifying what reinforces safe behaviors for a given workforce and building the systems that sustain those reinforcers over time.
Step 5: Assign Ownership, Resources, and Timelines
Every action item must have:
- A named owner (not a department)
- A realistic timeline
- Identified resources (budget, staff time, technology)
Without designated accountability, action plans drift. Use a simple action plan table format:
| Priority Dimension | Root Cause | Intervention | Owner | Completion Date | Success Metric |
|---|---|---|---|---|---|
| Nonpunitive Response to Error | Staff fear discipline when reporting | Leadership coaching on constructive feedback; policy revision clarifying just culture principles | Director of Safety | June 2026 | Near-miss reports increase 40%; dimension score improves from 38% to 55% |
Communicating Survey Results and Driving Buy-In
When employees participate in a safety culture survey and hear nothing back, the implicit message is clear: their input doesn't matter. Research confirms that organizations which communicate results and act on them see improvement in safety culture scores at reassessment; those that do not see scores stagnate or decline.
Communicating to Senior Leadership
Present findings in terms of business risk and operational impact, not just survey statistics:
- Connect low-scoring dimensions to incident trends, near-miss rates, or regulatory risk
- Quantify the cost of inaction (e.g., potential fines, workers' compensation claims, productivity loss)
- Show how improvement in specific dimensions (e.g., Management Support, Feedback/Communication) predicts overall safety performance
Leadership commits resources when they understand the stakes — frontline staff need a different kind of conversation entirely.
Communicating to Frontline Staff
Avoid clinical report-style presentations. Instead:
- Use plain language and department-specific data
- Provide a clear statement of what leadership commits to doing differently
- Hold small-group sessions rather than mass announcements so staff can ask questions
- Acknowledge what was promised after the last survey and what actually changed (transparency about past gaps is more effective at rebuilding trust than optimistic commitments alone)
The Role of Leadership Behavior
Leadership behavior is the most powerful signal employees receive about what is truly valued. If leaders want a reporting culture, their visible response to reported errors and near-misses has to reflect that.
Research on near-miss reporting confirms that management responses — positive reinforcement and constructive follow-up — determine whether a reporting culture is sustained or quietly abandoned.
Tracking Progress and Avoiding Common Pitfalls
Once your action plan is in motion, you need a system to measure whether it's actually working. Set up a progress tracking framework with three components:
Review cadence:
- Monthly check-ins on action item completion
- Quarterly reviews of leading indicators
Metrics tied to each goal:
- Voluntary incident reporting rates
- Near-miss reports submitted
- Supervisor behavior observation scores
- Safety huddle participation
Formal reassessment survey:
| Source | Recommended Interval |
|---|---|
| AHRQ | Every 12-18 months |
| The Joint Commission / Leapfrog | Annual measurement |
| CMS | Annual, or biennial if pulse surveys conducted between |
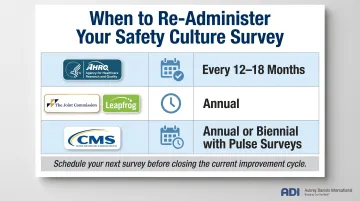
Use this table as your scheduling guide — book the next full survey administration before you close out the current improvement cycle.
Common Pitfall 1: Action Items With No Accountability
Problem: The action plan lists initiatives but no individual is named as owner.
When planning is done by committee, ownership often gets left ambiguous to avoid conflict — and nothing gets done.
Fix:
- Assign a single named owner to each action item (not a department)
- Build accountability checkpoints into leadership review meetings
Common Pitfall 2: Interventions That Target Awareness, Not Behavior
Problem: The organization responds to low scores with training sessions and policy updates, but survey scores don't improve at reassessment.
Training addresses what employees know — it doesn't change what they experience when they act safely or unsafely. The consequences of behavior drive the behavior itself.
Fix: Shift interventions toward changing behavioral consequences:
- Increase positive reinforcement for desired safe behaviors
- Ensure that reporting errors is met with constructive, non-punitive responses
- Make safe behavior the easier, more rewarding choice
Common Pitfall 3: Treating the Action Plan as a One-Time Event
Problem: The action plan is executed, but no reassessment is scheduled and improvement stalls after initial momentum.
This happens when safety culture improvement gets framed as a project rather than an ongoing process — one with a finish line.
Fix: Embed safety culture review into your organization's annual performance cycle. Each reassessment survey should serve as both an outcome measure and the starting point for the next improvement cycle.
Frequently Asked Questions
How do you create a safety action plan?
Start by analyzing survey results to identify priority dimensions, then conduct root cause analysis to understand behavioral drivers. Set SMART goals, design behavior-focused interventions that change antecedents and consequences, assign ownership with timelines, and schedule reassessment to measure progress.
What are good safety culture survey questions?
Effective safety culture survey questions assess key dimensions such as nonpunitive response to error, communication openness, teamwork, management support for safety, and organizational learning. AHRQ's HSOPSC and SOPS surveys are validated benchmarks that measure 12 composite dimensions across 42 items.
How to improve safety culture in healthcare?
Healthcare organizations improve safety culture by building voluntary error reporting systems, supporting a just culture where discipline is proportionate to intent, training teams in structured communication practices (such as SBAR), and using survey data to drive targeted behavioral interventions—not just policy updates.
What are the four C's of safety culture?
The four C's commonly referenced are Commitment (leadership dedication to safety), Communication (open, non-punitive information flow), Competence (skills and training to act safely), and Culture (shared beliefs and norms that shape daily safety behavior). James Reason's four-subculture framework covers similar ground and carries stronger research validation.
What are the 5 P's of patient safety?
The 5 P's—Patients, Professionals, Processes, Place (environment), and Patterns (data/learning)—provide a framework for identifying where safety improvements are needed.
Survey data only drives change when leaders treat it as a behavioral diagnostic, not a report card. Organizations that close the loop—linking scores to specific behaviors, assigning clear ownership, and measuring progress—see real shifts in how safety gets practiced day to day.