Introduction
Healthcare organizations operate in perpetual transformation—navigating regulatory updates, workforce shortages, evolving care models, and digital system implementations. Yet approximately 70% of all change management efforts fail. The problem rarely lies in strategy. Most initiatives falter because staff lack the motivation to sustain new behaviors beyond the initial rollout.
Creating a motivating work environment means deliberately engineering conditions—behavioral, structural, and cultural—that make people want to change and keep changing. That requires understanding the science of behavior, managing consequences systematically, and ensuring leadership actions reinforce desired behaviors every day.
The sections below cover the science behind sustained behavior change, the environmental elements that drive discretionary effort, and the leadership mistakes that derail even well-designed initiatives.
TLDR:
- Most healthcare change fails because organizations invest heavily in training and protocols (antecedents) but neglect the consequences that sustain behavior
- Motivation is an outcome of environment, not personality—leaders can engineer it through systematic reinforcement
- Discretionary effort (the gap between minimum and maximum performance) determines whether change sticks
- What leaders notice, reinforce, and respond to defines the actual motivational climate
Why Motivation Is the Missing Link in Healthcare Change
Healthcare change efforts typically follow a predictable pattern: invest in new protocols, purchase technology, design workflows, deliver training, announce rollout dates. Organizations excel at defining what needs to change and how to implement it. What they systematically underinvest in is the answer to why people will actually do it—the motivational environment that determines whether change survives contact with daily pressures.
The difference between compliance and genuine motivation determines success. Compliance produces minimum acceptable behavior—staff do just enough to avoid correction. A motivating environment generates discretionary effort: the extra commitment, problem-solving, and persistence that separates successful change from initiatives that fade under pressure.
Research analyzing 30,490 healthcare workers found that engaged staff (not merely compliant ones) produced measurably better safety outcomes, with engagement significantly associated with reduced errors and adverse events.
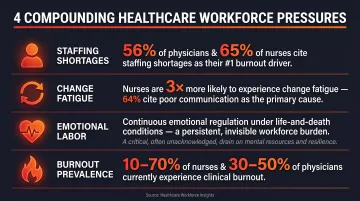
Healthcare's unique pressures intensify this challenge:
- Staffing shortages: 56% of physicians and 65% of nurses cite staffing shortages as the top contributor to burnout
- Change fatigue: Nurses are three times more likely to experience change fatigue than other healthcare professionals, with 64% identifying organizational communication as a key factor
- High emotional labor: Clinical work demands continuous emotional regulation while managing life-and-death consequences
- Burnout prevalence: Estimates range from 10-70% among nurses and 30-50% among physicians
Generic change management frameworks are designed for lower-stakes environments—they weren't built to account for these compounding pressures. Motivation must be built into the environment itself, not layered on through campaigns or one-time initiatives, because work conditions either consistently reinforce desired behaviors or steadily undermine them.
What Behavioral Science Tells Us About Motivation at Work
Applied Behavior Analysis (ABA) provides a foundational principle: behavior is a function of its consequences. In work environments, what gets reinforced gets repeated. What goes unreinforced—or worse, followed by negative consequences—gets extinguished, regardless of how thoroughly it was trained or communicated.
The ABC Model: Antecedents vs. Consequences
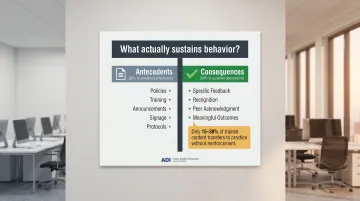
The ABC model (Antecedent-Behavior-Consequence) explains why most change initiatives start strong then fade:
- Antecedents set the occasion for behavior: policies, announcements, training sessions, signage, new protocols
- Behavior is the action itself
- Consequences determine whether behavior sustains: feedback, recognition, outcomes people experience
Most healthcare change programs are antecedent-heavy and consequence-light. Organizations invest thousands in training (an antecedent), then wonder why only 15-30% of trained content transfers to actual practice. Research confirms antecedents account for approximately 20% of sustained performance, while consequences account for 80%.
Positive Reinforcement: The Engine of Sustained Change
Positive reinforcement must be immediate, certain, and meaningful to the individual to be effective. Annual performance reviews and generic praise ("great job, everyone!") fail this test. What works:
- Specific behavioral feedback, delivered with context: "I noticed you closed the loop with the patient's family before discharge—that builds trust and prevents callbacks"
- Recognition delivered within hours or days, not weeks
- Peer acknowledgment, which is often more powerful than supervisor recognition alone
- Individualized reinforcement — what motivates one nurse (public recognition) may be aversive to another who prefers private acknowledgment
Discretionary Effort: The Performance Gap That Matters
Discretionary effort is the difference between the minimum an employee must do to keep their job and the maximum they're capable of contributing. This gap determines whether change initiatives succeed or regress to baseline. Only 20% of employees worldwide are engaged, meaning 80% are withholding discretionary effort.
A motivating environment consistently unlocks this gap. This principle underlies ADI's Performance Management methodology, developed over 45+ years of applied work across healthcare and other industries. Motivation is an outcome of the environment, not a fixed personality trait. Healthcare leaders can engineer it by systematically managing antecedents and consequences around the behaviors that matter most during change.
Key Elements of a Motivating Work Environment for Healthcare Change
Reinforce the Right Behaviors, Not Just the Right Outcomes
Outcomes lag behind behavior. By the time you see patient satisfaction scores or error rates, the opportunity to reinforce the specific behaviors that produced them has passed. Healthcare environments that motivate change build real-time feedback loops that catch and reinforce behaviors as they happen.
What this looks like practically:
- Leader rounding with behavioral specificity: Instead of "How's it going?" ask "Can you show me how you're using the new handoff protocol?" and recognize specific actions
- Structured peer recognition: Tie acknowledgment to observable actions, not personality ("Sarah is amazing" becomes "Sarah triple-checked the patient's allergy history before administering the new medication")
- Behavior-focused performance conversations: Pinpoint specific actions rather than generalizing about attitude or effort
When leaders focus exclusively on outcomes, they miss the daily behaviors that create those results. This also inadvertently reinforces the wrong behaviors: staff learn that only outcomes matter, regardless of the process used to achieve them.
Make Communication a Mechanism for Change, Not Just Information Transfer
In a motivating environment, communication is bidirectional and consequential. Staff need to see that their input visibly shapes decisions. When feedback disappears into suggestion boxes with no visible response, it teaches employees that speaking up doesn't matter. Research shows 64% of nurses identify organizational communication as a key factor influencing change fatigue.
How leaders make communication motivating:
Close the loop publicly:
- Share what feedback was heard: "Three units raised concerns about the new documentation time requirements"
- Explain what action was taken: "We've simplified the required fields and added scribes during peak hours"
- Acknowledge when constraints prevent action: "We can't change the regulatory requirement, but we can adjust staffing to support it"
Use structured huddles strategically:
- Celebrate early wins tied to specific behaviors: "Yesterday, the ED team completed 94% of handoffs using the new protocol—up from 67% last week"
- Focus on progress, not perfection
- Make success visible and attributable to specific actions
Separate information-sharing from problem-solving:
- Dedicate separate forums for each purpose
- Don't combine announcements with collaborative discussions—mixing them dilutes both
According to research on nurse resistance to change, communication barriers "ultimately affect the implementation, quality, and sustainability of change." Poor communication magnifies the negative aspects of change and creates uncertainty, while valid, timely communication significantly improves staff evaluation of change.
Build Psychological Safety Alongside Accountability
Psychological safety in change contexts means staff believe that raising concerns, trying new approaches, or making mistakes during implementation will not result in punishment or humiliation. Without it, staff revert to familiar behaviors because safety lies in the status quo.
The evidence is direct: higher-performing hospital teams reported higher error rates, not because they made more mistakes, but because psychological safety enabled them to discuss errors openly.
That openness matters at every level. 68.9% of nurses express unwillingness to report their own medication errors, primarily due to fear of punitive responses.
Critical principle: Psychological safety and accountability are not opposites—they're complementary. A motivating environment holds people accountable through positive reinforcement of desired behaviors, not punishment of errors. This balance sustains the risk-taking and learning essential during change.
Practical application:
- Distinguish human error (addressed through system redesign) from reckless behavior (addressed through consequences)
- Respond to early-stage mistakes during change with coaching, not correction
- Recognize staff who identify problems or near-misses
- Make "I don't know yet" or "I need help" acceptable responses during learning curves
The just culture framework—balancing accountability with psychological safety—prevents the phenomenon where punitive responses to early change-related errors teach staff that innovation is dangerous.
How Leadership Behavior Shapes the Environment for Change
The work environment is largely a reflection of leader behavior. How leaders respond (or fail to respond) to staff behaviors—what they notice, what they reinforce, what they ignore, what they criticize—shapes the actual motivational climate, regardless of posted values or stated priorities.
Gallup research finds that managers account for at least 70% of the variance in employee engagement across business units. Similarly, a Mayo Clinic study found that leadership quality explained almost 50% of the variation in physician satisfaction scores. Leadership behavior is the primary determinant of whether change takes root.
Behavioral Leadership: Making Leader Behavior Deliberate
Behavioral leadership means leaders are deliberate about:
- Observing specific staff behaviors during change: Not just checking off compliance boxes, but watching for the actual behaviors that drive outcomes
- Providing immediate, specific positive feedback: "I saw you validate the patient's understanding before moving to the next step—that's exactly the patient-centered approach we're building"
- Removing obstacles that punish desired behaviors: If the new documentation process takes longer and there's no acknowledgment of the extra effort, the environment inadvertently punishes adoption

Example: A hospital implements a new handoff protocol requiring structured communication. If leaders never observe handoffs, never recognize staff using the protocol well, and only comment when handoffs are missed, they've created an environment where the new behavior receives no positive consequences. Staff learn the safest approach is minimal compliance.
The Risk of Extinction in Change Efforts
In behavioral science, extinction occurs when reinforcement maintaining a behavior stops, causing the behavior to gradually disappear. In change initiatives, this happens when leaders champion a new initiative at launch then go silent: no follow-up recognition, no visible engagement with progress, no reinforcement for adoption. The motivating energy dissipates rapidly.
Common signs a change effort is entering extinction include:
- Staff revert to old workflows despite initial adoption
- Only the most compliant employees continue using the new process
- Questions about the initiative stop — no one asks because no one expects a response
As Dr. Aubrey Daniels writes, "Change that does not build in feedback and positive consequences for the new behavior is not sustainable." Leadership attention to behavior is not optional. It is the mechanism that keeps change alive.
Leadership Development for Sustainable Change
Leadership development for change must focus on behavior-based coaching skills—how to observe, pinpoint, and reinforce specific staff behaviors—not just how to communicate a vision or manage project timelines. Leaders need training in:
- Pinpointing observable behaviors that drive desired outcomes
- Delivering timely, specific positive reinforcement
- What individually motivates each team member (reinforcement is not one-size-fits-all)
- Building feedback systems that make progress visible
- Catching small wins and early adoption before momentum fades
Without these skills, even well-intentioned leaders default to antecedent-only management: announcing, training, reminding. They set up the conditions for change but never reinforce the behaviors that make it stick. In healthcare, where staff are already stretched, that gap is the difference between a change effort that lasts and one that quietly disappears.
Common Mistakes That Undermine Motivation During Healthcare Change
The Announcement-to-Abandon Pattern
Organizations launch change with high-energy kickoffs, training sessions, posters, and clear goals. Then leader attention shifts to the next priority—leaving staff without the reinforcement needed to sustain new behaviors. The environment reverts because consequences were never redesigned.
This pattern is common — and costly. Initial training provides antecedents (triggers for behavior), but without sustained support, trained behaviors extinguish. Staff conclude the initiative wasn't really a priority.
What's typically missing after launch:
- Ongoing leader attention and follow-through
- Peer recognition tied to new behaviors
- Visible progress tracking
- Positive consequences for early adoption
Punitive Accountability During Learning Curves
When errors during change implementation are met with criticism or corrective action before the new behavior is established, staff learn that change is risky. In healthcare cultures with strong perfectionism norms, this dynamic is especially damaging.
Research on just culture found that managerial inconsistency in addressing errors—handling similar incidents differently—creates perceptions of unfairness that discourage reporting and participation in safety initiatives. The solution is shifting from retributive justice (penalizing individuals) to restorative approaches that focus on system learning and improvement.
In motivating environments, early mistakes are expected and met with coaching. Punitive responses during learning curves don't improve performance — they drive behavior underground.
Uniform Motivation Strategies
What reinforces one nurse (public recognition in team meetings) may be aversive to another (who finds public attention uncomfortable). A motivating environment requires leaders to understand what is individually reinforcing—a skill that demands deliberate development, not intuition.
Common mistake: Implementing organization-wide recognition programs (e.g., monthly awards, public announcements) without considering individual preferences. Some staff respond positively; others avoid the behaviors that trigger recognition.
Better approach:
- Ask staff directly what types of recognition they value
- Observe what consequences naturally follow high performance for different individuals
- Offer multiple recognition pathways (public acknowledgment, private notes, peer nominations, informal verbal feedback)
- Train leaders to individualize reinforcement strategies
One-size-fits-all programs waste resources — and miss the staff whose discretionary effort is most available, if only someone asked what actually motivates them.
Frequently Asked Questions
How to create a positive work environment in healthcare?
Creating a positive environment in healthcare requires deliberately reinforcing behaviors that reflect desired values through specific feedback, meaningful recognition, and leadership that models the cultureinstead of relying on policy changes or one-time training alone. The environment must systematically deliver positive consequences for desired behaviors.
What are the 5 C's of motivation?
The 5 C's — Challenge, Curiosity, Confidence, Control, and Collaboration — represent conditions that support engagement and intrinsic motivation. In behavioral terms, each factor creates the environment needed for positive reinforcement, autonomy, and meaningful contribution to take hold and increase discretionary effort.
What is the biggest barrier to motivation during healthcare change?
The gap between initiating change (training, policy rollout) and sustaining it (reinforcement, feedback) represents the biggest barrier. Most motivation fades because organizations invest in antecedents but neglect the ongoing positive reinforcement that maintains behavior change over time.
How does positive reinforcement apply in a healthcare work environment?
Positive reinforcement means immediately and specifically acknowledging behaviors that support quality care or change adoption — not just end results — so staff are more likely to repeat them. To work, it must be timely (within hours or days), specific to the exact behavior observed, and meaningful to the individual receiving it.
Why do change initiatives in healthcare often fail to stick?
Change fails when the environment continues to reinforce old behaviors (or fails to reinforce new ones), leader attention drifts after launch, and accountability focuses on punishing mistakes rather than reinforcing progress. Without systematic consequence management, trained behaviors naturally extinguish over time.
How can leaders measure whether their work environment is motivating staff?
Behavioral indicators provide more meaningful measures than engagement survey scores alone. Watch for discretionary effort, voluntary adoption of new practices, how often staff seek feedback, and whether staff raise concerns or try new approaches without prompting — these signal a genuinely motivating environment.
A motivating work environment for healthcare change is built, not inspired. When leaders understand behavioral science, manage consequences deliberately, and reinforce the right actions consistently, motivation becomes a measurable capability — one that outlasts any single initiative or announcement.