Introduction
More than 3 million deaths occur annually worldwide due to unsafe healthcare, and more than half of this harm is preventable. It persists anyway. According to the WHO's 2023 Patient Safety Fact Sheet, approximately 1 in 10 hospitalized patients is harmed during care. The scale of preventable patient harm has forced healthcare leaders to confront an uncomfortable truth: clinical protocols and technology alone cannot solve this crisis. Organizational culture — the collective beliefs, attitudes, and daily behaviors of staff — shapes safety outcomes as directly as any procedure manual.
The Patient Safety Climate in Healthcare Organizations (PSCHO) survey offers healthcare leaders a validated, evidence-based instrument to measure safety climate across organizational, work-unit, and interpersonal levels simultaneously. This article covers what the PSCHO survey measures, how to administer and interpret it, and how to translate scores into behavioral change that protects patients and staff.
TLDR:
- The PSCHO survey measures patient safety climate across three levels: organizational, work-unit, and interpersonal
- Validated across 99 hospitals, the PSCHO surfaces gaps in leadership commitment, error reporting, and teamwork
- Perception of management consistently scores lowest across global safety climate studies — making leadership behavior the highest-yield intervention target
- Effective administration requires psychological safety; interpretation hinges on spotting role-based perception gaps
- Measurement alone does not improve safety. Behavioral interventions must follow survey results to create sustainable change
What Is Patient Safety Climate — and Why It's Hard to Measure
Defining Patient Safety Climate
Patient safety climate is the collective perception of how seriously an organization prioritizes safety at a given moment. Unlike safety culture—the deeper, slower-to-change set of shared values and norms—safety climate functions as a snapshot of staff sentiment captured at a specific point in time. It reflects what employees believe leadership values, how safe they feel reporting errors, and whether they trust their colleagues to prioritize patient safety.
Why Measurement Is Difficult
Safety climate is inherently invisible: a pattern shaped by fears, hierarchies, and trust that no policy document can fully capture. Survey design and psychological safety both heavily influence data quality. A systematic review of 30 studies found that 63% identified fear of consequences as the leading barrier to error reporting.
Even when surveys promise anonymity, staff may still fear blame, punishment, or job loss — and that fear quietly distorts the data.
Hierarchy dynamics further complicate measurement. Senior leaders consistently perceive safety climate more positively than frontline staff. This perception gap means organizational leaders may believe safety is prioritized when frontline nurses, technicians, and physicians experience the opposite reality daily.
Choosing the Right Instrument Matters
That measurement challenge makes instrument selection critical. Multiple validated tools exist, each designed for different organizational contexts:
| Instrument | Primary Design Context | Level of Analysis |
|---|---|---|
| PSCHO | VA + private hospitals, organizational benchmarking | Organizational + Work-unit + Interpersonal |
| SAQ (Safety Attitudes Questionnaire) | ICU, OR, inpatient units | Unit/clinical area |
| AHRQ HSOPSC | General hospital settings | Unit + Hospital |
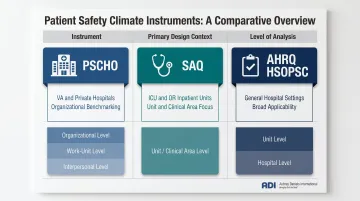
Selecting the wrong tool produces data that doesn't fit your organizational structure — or your improvement goals. The PSCHO captures variance across all three levels simultaneously, which makes it the right choice when leadership accountability and systemic gaps are the primary focus.
The PSCHO Survey: Origins, Purpose, and What Sets It Apart
Development and Validation
The PSCHO survey was developed by Benzer, Meterko, and Singer and published in the Journal of Evaluation in Clinical Practice in 2017.
The instrument was validated across 99 hospitals (69 private-sector facilities and 30 Veterans Health Administration hospitals), surveying senior managers, physicians, and a random 10% sample of all other hospital personnel.
The short-form PSCHO (15 items) was specifically designed to reduce respondent burden while maintaining the variance captured by the original 38-item version. Psychometric validation confirmed strong reliability, with organizational-scale coefficients around 0.84 and a three-factor structure validated through confirmatory factor analysis.
What Makes the PSCHO Distinct
The PSCHO uniquely measures patient safety climate across three distinct levels:
- Organizational Level: Covers leadership commitment to safety, resource allocation, and the facility's overall safety emphasis
- Work-Unit Level: Addresses unit management support, safety norms, risk recognition, collective learning, and psychological safety
- Interpersonal Level: Captures fear of shame and fear of blame or punishment when errors occur
This multilevel design distinguishes the PSCHO from instruments like the SAQ (which focuses primarily on unit-level attitudes derived from aviation safety research) and the AHRQ HSOPSC (which captures unit and hospital levels but does not explicitly model interpersonal fear dynamics).
The PSCHO was developed and validated within the VA healthcare system and then extended to private-sector hospitals, giving it broader population validity than single-system instruments.
Intended Use Cases
The PSCHO is best suited for organizations seeking to:
- Establish a baseline safety climate before launching culture transformation initiatives
- Benchmark safety climate changes over time following interventions
- Identify systemic gaps in leadership support, error reporting norms, or teamwork quality before designing improvement programs
- Understand organizational-level variance that unit-focused tools cannot capture
The Six Dimensions the PSCHO Survey Measures
Framework Overview
The PSCHO measures patient safety climate across multiple dimensions that reflect both individual attitudes and organizational systems. Understanding each dimension helps leaders pinpoint where to focus improvement efforts. While the PSCHO's formal structure includes organizational, work-unit, and interpersonal levels with approximately 10 subdimensions, it shares conceptual grounding with widely validated tools like the Safety Attitudes Questionnaire (SAQ).
Teamwork Climate
How well staff collaborate—and whether they trust each other to communicate clearly—is what this dimension captures. Poor teamwork is a major risk factor for patient harm. A 10-year analysis of trauma morbidity and mortality conferences found communication errors were the most frequent error type, accounting for 29 of 130 identified errors—and 72% of communication failures led to subsequent sequential errors such as missed diagnoses and under-triage.
When staff do not trust colleagues to share critical information or collaborate effectively, patient safety erodes rapidly.
Safety Climate and Error Reporting
This dimension measures staff perception that the organization proactively prioritizes safety. Error reporting is a critical subdimension—organizations with punitive cultures suppress reporting, cutting off the feedback loop needed for systemic correction.
The IOM's landmark To Err Is Human established that most medical errors stem from faulty systems and conditions, not individual negligence. Yet 63% of studies identify fear of consequences as the primary barrier to reporting. When leaders focus on individual fault rather than system failures, reporting rates drop and organizations lose the data they need to improve.
Job Satisfaction, Stress Recognition, and Working Conditions
These three dimensions form a "human factors" cluster:
- Job Satisfaction — Whether staff feel positive about their work experience and believe their contributions are valued
- Stress Recognition — Whether staff acknowledge how fatigue and stress impair their own performance (research shows newer staff often score higher here, as experienced staff may habituate to chronic stress)
- Working Conditions — Staffing levels, equipment adequacy, logistical support
Working conditions consistently score among the lowest dimensions across global studies. Resource constraints—understaffing, inadequate equipment, unsustainable workloads—directly increase error risk regardless of individual competence or motivation.
Perception of Management
Staff trust in management—at both the unit and hospital level—is what this dimension measures. Across multiple international studies, perception of management receives the lowest positive scores among all safety climate dimensions.
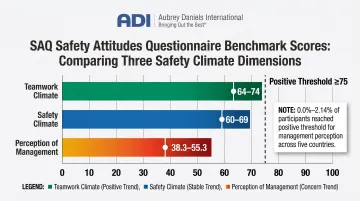
SAQ benchmark data across 10,843 respondents in 203 clinical areas showed Perception of Management scoring between 38.3 and 55.3 on a 0-100 scale—far below teamwork climate (64-74) and safety climate (60-69). An international study across five countries found that only 0.0% to 2.14% of participants reached a "positive" threshold (score of 75 or higher) for this dimension.
That finding is consistent across borders and healthcare settings. Leadership engagement is the most reliable intervention target for safety climate improvement.
How to Administer the PSCHO Survey Effectively
Pre-Administration Decisions
Choosing the Version:
- Short-form (15 items) — Reduces survey fatigue, ideal for repeated measurement and busy clinical settings
- Full version (38 items) — Provides more granular data, suitable for comprehensive baseline assessments
Target Population:
- All clinical staff vs. specific units
- Include senior management, physicians, nurses, technicians, and administrative staff for multilevel analysis
Administration Mode: Electronic surveys enable faster data analysis and preserve anonymity but may reduce response rates. Research shows face-to-face administration achieves 71.7% average response rates, while web-based methods are negative predictors of participation.
The PSCHO short form addresses survey length concerns, but the chosen mode must still balance convenience with response quality.
Building Psychological Safety Before Launch
Set expectations upfront so staff understand:
- Responses are anonymous and will not be traced to individuals
- Results will be used to improve systems, not punish staff
- Leadership is committed to acting on findings
Staff trust in confidentiality is a precondition for valid data. Leadership messaging before administration directly affects both response rates and candor — without it, even a well-designed survey produces unreliable results.
Practical Administration Steps
- Assign facility-level survey coordinators to manage reminders and ensure access
- Set a defined administration window (typically 2-3 weeks)
- Provide periodic participation reminders without creating survey fatigue
- Plan a structured data review process before administering the survey, so staff see results translate into action

One more step worth taking before launch: clarify whether the survey is intended for internal benchmarking or external research comparison. The scope differs meaningfully, and a clear purpose statement prevents confusion when other surveys are running concurrently.
Interpreting PSCHO Results: Patterns, Benchmarks, and Red Flags
Scoring Framework
The PSCHO typically uses a Likert scale, with scores converted to percentage-positive metrics. For example, the SAQ convention treats scores ≥75 as "positive." This threshold helps leaders distinguish high-performing dimensions from those requiring urgent attention.
PSCHO-specific benchmarks from a 30-hospital VA study reported:
- Mean Percent Problematic Response (PPR): 17.5% (lower PPR indicates better climate)
- Range across hospitals: 12.0% to 23.7%
- Senior managers reported the lowest PPR (most positive perceptions)
- Frontline staff and high-hazard units (OR, ICU, ED) reported significantly higher PPR
Common Patterns Across Settings
Across European, North American, and Asian healthcare settings:
- Perception of management and working conditions are consistently the weakest-scoring dimensions
- Stress recognition tends to score highest
- Teamwork climate is the strongest predictor of overall safety climate
Regression analysis from Indian hospitals found Teamwork Climate (coefficient: 0.219, p<0.001) and Perception of Management (coefficient: 0.077, p=0.022) were the only statistically significant predictors of overall Patient Safety Index.
Demographic Variables and Interpretation
Professional role, years of experience, department type, and facility context all produce meaningful score differences:
- Senior managers perceive safety more positively than frontline staff
- Clinicians report lower safety climate than non-clinicians
- High-hazard units (OR, ICU, ED) report lower safety climate than other areas
- Newer staff often score higher on stress recognition
When senior leaders score safety climate far higher than frontline nurses, that gap points directly to where intervention is needed — between written policy and daily practice.
Key Red Flags Requiring Immediate Attention
- Extremely low perception of management scores — Staff do not believe safety is a genuine organizational priority
- Very low working conditions scores — Resource constraints directly increase error risk
- Near-zero positive scores on error reporting — Punitive culture actively suppresses the information organizations need to improve
A scoping review of 34 studies found 76% reported statistically significant associations between higher patient safety culture scores and reduced adverse event rates. When safety climate scores are low, adverse events are more likely.

Internal Benchmarking Over External Comparisons
Knowing where the red flags are raises an immediate question: compared to what? The most reliable answer is your own baseline. The primary value of the PSCHO is tracking change over time — hospital size, patient mix, staffing models, and regional factors make external comparisons misleading. Measure whether interventions move scores in the right direction. That's the standard that matters.
From Survey Scores to Sustainable Change: The Behavioral Science Approach
Survey Scores Are Diagnostic, Not Prescriptive
Knowing that teamwork climate or management perception scores are low tells you where the problem is—not what specific behaviors need to change or why staff currently behave as they do. The next step requires understanding the behavioral antecedents and consequences that maintain current safety-relevant behaviors.
Effective Follow-Through From a Behavioral Science Perspective
Organizations must identify which specific behaviors are being suppressed by punitive consequences or a lack of positive reinforcement, then redesign the environment so safe behaviors are reinforced rather than punished. Common suppressed behaviors include:
- Speaking up about errors or near-misses before they escalate
- Following handoff protocols consistently under time pressure
- Reporting unsafe conditions without fear of blame or retaliation
Once identified, the goal is to redesign the organizational environment so safe behaviors are reinforced rather than punished.
ADI applies this approach through frameworks like Safe by Accident? (co-authored by Judy Agnew and Dr. Aubrey Daniels). The method focuses on identifying the smallest behavior change that produces the biggest safety impact, then using targeted coaching and feedback to sustain it.
Leadership Behavior Sustains Change
PSCHO scores on management perception and safety climate directly reflect what leaders consistently model and reinforce. Lasting improvement shows up in what leaders actually do: responding to error reports without blame, making time for safety conversations during routine rounds, and removing the procedural obstacles that make safe behavior harder than unsafe behavior.
PSCHO data consistently shows management perception as the lowest-scoring dimension worldwide — which means leadership behavior change is also the highest-yield intervention target. When leaders act on what staff report rather than simply acknowledging it, perceptions shift in measurable ways.
The Risk of Survey Fatigue and Performative Compliance
If staff complete the PSCHO survey and see no action taken on results, trust erodes and future survey data becomes less reliable. Research on response rates documents that healthcare settings in high-income countries experience declining participation, attributed to habituation and a perception that surveys "do not result in meaningful changes."
Closing the feedback loop—communicating what was found and what will change—is as important as the survey itself. Without that follow-through, the next survey cycle starts with staff already skeptical of the process.
Frequently Asked Questions
What is the difference between the PSCHO survey and the SAQ?
Both are validated patient safety climate instruments, but the PSCHO measures safety climate at the organizational level and was validated within large integrated health systems (VA and private hospitals), while the SAQ focuses on unit-level safety attitudes and was originally developed for ICU and operating room settings.
What dimensions does the PSCHO survey measure?
The PSCHO measures teamwork climate, safety climate, job satisfaction, stress recognition, perception of management, and working conditions. These dimensions span organizational, work-unit, and interpersonal levels, capturing both individual attitudes and systemic factors.
How is patient safety climate different from patient safety culture?
Safety climate is a snapshot of current staff perceptions and attitudes, while safety culture is the deeper, more stable set of shared values and norms. Climate is measurable with surveys at a point in time; culture changes more slowly through sustained behavioral and leadership shifts.
What does a low score on "perception of management" indicate?
Low management perception scores indicate staff do not believe leadership actively supports patient safety at their unit or hospital level. Research links this to reduced error reporting, lower staff engagement, and higher risk of adverse events.
How often should a healthcare organization administer the PSCHO survey?
Periodic administration—such as annually or following major organizational changes or interventions—allows organizations to track whether safety climate is improving over time. Repeated measurement reveals whether interventions are working, which a single administration cannot show.
Final Insight:
The PSCHO survey is a powerful diagnostic tool. Measurement alone, however, changes nothing. The value lies in what leaders do after they receive the data. Organizations that translate scores into specific behavioral interventions, model safety commitment daily, and build non-punitive reporting cultures see climate scores rise and patient harm decline. Organizations that survey without acting see trust erode and scores stagnate — the data itself is not the intervention.
If your organization is ready to move from measurement to meaningful change, contact Aubrey Daniels International at 1-678-904-6140 or info@aubreydaniels.com to learn how behavioral science can drive measurable, lasting improvements in your safety culture.