This guide is written for healthcare administrators, quality improvement leaders, and clinical operations managers who need a systematic, science-backed approach to sustainable provider behavior change. Most organizations treat this as a training or policy problem. It isn't. It's a behavioral science problem — and the solution requires a fundamentally different framework.
The six steps outlined here draw on behavioral science research to help you diagnose, design, and sustain provider behavior change that actually holds.
TL;DR
- Aligning provider behavior requires a behavior-specific, structured approach — not just more education
- The six steps: define target behaviors, identify provider groups, diagnose behavioral drivers, involve providers in design, match interventions to drivers, and monitor holistically
- Most initiatives fail because organizations skip diagnosis and default to generic training
- Positive reinforcement outperforms compliance-only approaches for durability
- Sustainable alignment depends on continuous feedback loops — one-time interventions rarely hold
What "Aligning Provider Behavior with Best Practices" Actually Means
Before designing any intervention, three distinctions determine whether your approach will actually work.
Provider behavior refers to specific, observable actions during care delivery: clinical decisions, documentation habits, handoff communication, protocol adherence. Intentions and attitudes don't count. What a provider actually does is the unit of analysis.
Best practices means evidence-based clinical guidelines, care protocols, regulatory requirements, and organizational standards that represent the highest-quality approach to care. These are operationally defined, not abstract ideals.
Alignment vs. compliance is the sharpest distinction of the three. Compliance is minimum adherence driven by rules and fear of consequences. Alignment reflects internalized behavior change — providers consistently choose best-practice behaviors because the environment reinforces those choices. This distinction shapes every intervention decision that follows.
Why Provider Behavior Alignment Is Critical
Provider behavior is the single greatest variable in care quality. The evidence is hard to ignore:
- Adherence to recommended care processes in the U.S. sits near 50% across many clinical domains
- Preventable adverse drug events from injectable medications affect roughly 1.2 million inpatient hospitalizations annually, with 73% of ADE-related cases deemed preventable and national costs estimated at $2.7–$5.1 billion
- A 2024 study on community-acquired pneumonia found that while 91.6% of providers started antibiotic treatment within 48 hours, only 20.2% adhered to guideline-recommended treatment duration — two behaviors, one protocol, vastly different adherence rates

These gaps aren't random. They're predictable consequences of deploying one-size-fits-all training without understanding why providers behave the way they do.
What Goes Wrong Without a Structured Approach
Organizations typically see a recognizable pattern: a performance gap is identified, training is deployed, behavior improves briefly, then reverts within weeks. Leadership attributes this to provider resistance or motivation problems. The actual cause is more straightforward: the behavioral drivers were never diagnosed, and the consequence structure never changed to sustain the new behavior.
The Six Steps to Align Provider Behavior with Best Practices
These six steps function as an integrated process. Skipping any one of them weakens everything that follows.
Step 1: Define the Specific Behaviors You Want to Change
"Improve guideline adherence" is not a behavior — it's an outcome. The first step is breaking that outcome into discrete, observable, measurable actions.
Consider what the pneumonia research illustrates: treatment initiation and treatment duration are two separate behaviors within a single protocol. Reporting one global "adherence rate" masks which sub-behavior is failing. The same logic applies to sepsis bundles, discharge checklists, or any complex protocol.
To define target behaviors:
- Map every sub-behavior in the clinical process
- Identify where breakdowns actually occur (not where you assume they occur)
- Select the 2–3 priority sub-behaviors with the largest gaps
- Write each behavior in observable, measurable terms

Vague targets produce vague interventions — and vague interventions produce no measurable change in the behaviors that matter.
Step 2: Identify the Specific Provider Groups to Target
Provider behavior varies significantly across roles, care settings, and experience levels. Physician hand hygiene compliance runs at a median of 32% versus 48% for nurses, and ICU compliance drops further under high-workload conditions. These aren't minor differences — they point to distinct intervention needs.
Generic, organization-wide rollouts dilute impact and waste resources. Targeting by role, care setting, workload intensity, and measured performance gap concentrates resources where behavioral change will have the greatest clinical and operational effect.
Useful segmentation dimensions include:
- Role (physician vs. nurse vs. technician)
- Care setting (ICU vs. general ward vs. ambulatory)
- Patient volume or workload intensity
- Measurable performance gap size
Step 3: Diagnose the Factors Driving Current Behavior
Most intervention failures trace back to this step being skipped entirely.
Before designing anything, you need to understand why providers behave as they currently do. ADI's PIC/NIC Analysis® is one useful tool here: it identifies whether unintended positive consequences are reinforcing wrong behaviors or unintended negative consequences are suppressing desired ones. The broader ABC model (Antecedents, Behavior, Consequences) provides the same diagnostic structure.
Common behavioral drivers that require different solutions:
| Driver | What It Looks Like | What It Requires |
|---|---|---|
| Knowledge gap | Provider doesn't know the protocol | Targeted education |
| Workflow friction | EHR requires 6 clicks to document compliance | Process/tool redesign |
| Competing priorities | Correct behavior adds time under pressure | Task simplification |
| Consequence gap | Doing the right thing goes unnoticed | Structured reinforcement |
| Social norms | Peer behavior models non-adherence | Norm-shifting strategies |
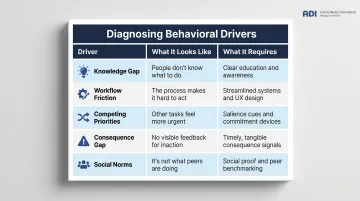
Research on hand hygiene noncompliance found that 44% of missed opportunities were attributable to memory, attention, or decision-making problems — not ignorance. Meanwhile, U.S. physicians rate EHR usability at a median score of 45.9 out of 100 (bottom 9% of all software systems). These are structural and environmental problems. Training won't solve them.
Step 4: Involve Providers in the Design of Interventions
Interventions designed without frontline input are often technically correct but operationally unworkable. Providers know where the friction actually lives — and that knowledge is invisible to administrators working from data alone.
ADI's Behavioral Roadmapping process exemplifies this approach: consultant-facilitated sessions engage frontline staff and high performers to reverse-engineer from desired outcomes to the specific behaviors required at each level.
In one case, those sessions surfaced something no policy review had caught — workers had quietly eliminated safety steps they considered redundant. The resulting conversation led to a mutually redesigned procedure that held.
The level of involvement doesn't need to be elaborate. Even basic consultation — asking providers what makes the target behavior harder than the alternative — surfaces barriers that no amount of policy review will catch.
Step 5: Match Interventions to the Actual Drivers of Behavior
Defaulting to education regardless of the diagnosis is the costliest mistake in this process. If the driver is a workflow barrier, training doesn't fix it. If the driver is a consequence gap, a new policy won't either.
Match the intervention to what the diagnosis actually shows:
- Knowledge gap → Focused, high-engagement training (not passive lecture)
- Workflow/tool barrier → Process redesign, environmental restructuring
- Competing priorities → Reduce task complexity, clarify expectations
- Consequence gap → Structured positive reinforcement and corrective feedback
ADI's Performance Management approach addresses the consequence gap directly. Rather than relying on compliance pressure, the methodology uses measurement, feedback, and positive reinforcement — applied systematically and in sequence — to make best-practice behaviors the default, not the exception. The approach treats positive reinforcement not as a nice-to-have but as the primary driver of durable behavior change.
Research on social norm and credible-source feedback supports this: credible-source feedback improved guideline adherence with a rate difference of 0.12 (95% CI 0.06–0.19). The VA hypertension study found that only interventions targeting time pressure and task complexity improved performance — while reminders and feedback deployed without attention to the actual driver had no effect.
Combining approaches strategically amplifies impact. Supportive supervision paired with peer mentorship addresses both the environmental and social reinforcement dimensions simultaneously.
Step 6: Use Holistic Monitoring and Evaluation
Measuring outcomes alone won't tell you whether the behavior changed. A reduction in readmissions doesn't confirm that discharge protocols are being followed — it just shows a downstream result.
Track behavior change across multiple data sources:
- Direct observation (did the provider perform the specific action?)
- Audit-and-feedback data tied to discrete sub-behaviors
- EHR-derived behavioral taxonomies (which steps in the protocol were completed or skipped)
- Provider self-report for context and barriers
- Patient experience data as a secondary indicator
Document how the intervention evolved and how your team tailored it to different provider subgroups. Without that implementation record, successful approaches can't scale — and failed ones tend to get repeated.
Key Factors That Affect Provider Behavior Change
The six steps provide a framework, but these contextual factors determine whether the changes actually stick:
- Training format matters more than duration. Fluency-based approaches — which build accuracy and speed through repeated practice rather than passive instruction — produce faster skill transfer. ADI's work with a medical insurance company reduced training duration by 34% while new hires reached seasoned-employee performance levels in 3 weeks instead of 26.
- Role-specific delivery outperforms broadcast rollouts. Smaller, targeted sessions increase relevance and retention.
- Financial incentives alone are insufficient. Pay-for-performance can shift behavior, but providers are more sustainably driven by quality-of-care purpose and peer recognition. Incentives work best paired with non-financial reinforcement.
- Leadership modeling is a multiplier. When clinical leaders visibly practice best-practice behaviors and publicly recognize providers who do the same, they shift the social norm — a mechanism that research consistently identifies as more durable than policy mandates or financial pressure alone.
- Multifaceted isn't always better. The evidence supports both single-component and bundled approaches. The deciding factor is whether the intervention targets the actual behavioral driver, not how many components it includes.
Common Mistakes Organizations Make
Treating behavior alignment as a knowledge problem. Consider hand hygiene: providers know the protocol. Compliance still sits well below 50% in most settings. The real barrier is context, not awareness. Doing the right thing is slower and less convenient, and it rarely gets acknowledged. Under time pressure, the path of least resistance wins every time.
Deploying solutions before diagnosing the problem. Jumping to an intervention without understanding why the gap exists is the most expensive mistake in behavior change. The result is predictable: behavior improves briefly, then reverts. Without identifying the actual driver, no intervention can be designed to address it.
Running a project instead of building a practice. ADI's work across 400+ companies shows that positive reinforcement must be embedded in daily management, not scheduled as an annual training event. Organizations that treat alignment as a project will see regression toward old behaviors once the intervention ends.
Frequently Asked Questions
What are examples of health behavior interventions?
Common types include education and training, audit-and-feedback mechanisms, clinical decision support tools, peer mentorship, supportive supervision, financial incentives, and environmental redesign. The most effective approaches combine multiple components matched to specific behavioral drivers rather than defaulting to a single method.
What are the 5 A's of behavior change?
The 5 A's (Assess, Advise, Agree, Assist, Arrange) originated as a provider-facing patient counseling framework. The principle applies equally to designing provider behavior interventions: diagnosis precedes prescription, whether you're working with patients or clinicians.
Why do providers fail to follow clinical best practices?
Most often it isn't ignorance. Workflow friction, competing priorities, unclear accountability, and the absence of positive reinforcement for doing the right thing are the primary drivers. Knowledge alone rarely predicts behavior when the environment doesn't support the desired action.
How do you measure provider behavior change?
Use direct observation, audit-and-feedback data, EHR-derived behavioral taxonomies, and provider self-report. Measuring whether the provider performed the specific action is more actionable than measuring outcomes alone — outcomes can shift for reasons unrelated to the behavior you targeted.
What is the role of reinforcement in changing provider behavior?
Positive reinforcement — recognizing and rewarding best-practice behaviors promptly and specifically — is the most durable driver of behavior change. Compliance-only approaches may produce short-term results but tend to increase disengagement over time. ADI recommends making reinforcement a daily practice, not an occasional event.
What is the role of reinforcement in changing provider behavior?
Positive reinforcement, meaning recognizing and rewarding best-practice behaviors promptly and specifically, is the most durable driver of behavior change. Compliance-only approaches may produce short-term results but tend to increase disengagement over time. ADI recommends making reinforcement a daily practice, not an occasional event.
How long does behavior change last after a training intervention?
Without ongoing reinforcement, behavioral gains from training typically fade quickly. ADI's position, grounded in Applied Behavior Analysis, is that sustained behavior change requires continuous environmental support: measurement, feedback, and positive reinforcement applied systematically over time. Training alone is not enough.